Author: Julie Donnelly, LMT – The Pain Relief Expert
Editor: Dr. Steve Chaney
While February is the shortest month of the year, to our northern family and friends it is the longest, seemingly endless, month because it seems like winter is never going to go away.
Where I live in Sarasota Florida, winter brings us near-perfect days and cooler nights. It’s my favorite time of year. And of course, we all celebrate the holiday of love – Valentine’s Day!
Just a bit of trivia: In 1868, Richard Cadbury released the first Valentine’s Day box of chocolates, followed in 1902 with the first Valentine hearts from the New England Confectionery Company. In the 1840s, Esther A. Howland created the first commercial Valentine’s Day cards in the United States. Hallmark first offered Valentine’s Day cards in 1913 and began producing them in 1916. (Thanks to Wikipedia for all this interesting info).
I was reviewing last year as I was deciding on a topic for this month. We discussed:
*Heel pain
*Groin pain
*Low back pain
*Restless leg
*Foot pain
*We spent two months discussing various causes of headaches,
*And now we are in 2024, this will be the second month explaining some of the many causes of knee pain.
In each of these I showed, or explained to you, how to do a simple self-treatment that can help to relieve the pain. Each of the treatments are in my books, and many people have decided to just order one of the books, so they had the full treatment protocol for aches and pains from your head to your foot.
I’ve done self-treatment videos, and if you have come to the office, you know that I teach you how to do specific self-treatments that relate to your personal area of pain.
Before I change the way I do things, let’s finish off knee pain by talking about a little muscle that causes pain deep inside your knee joint. It’s a muscle called popliteus.
Your Popliteus Muscle And Knee Pain
The popliteus is a small muscle that causes a LOT of deep-knee pain. It is located at the back of your knee joint. It attaches to the bone in your lower leg, crosses the joint, and inserts into your thigh bone. You can get a good look at it and read all about it by going to https://en.wikipedia.org/wiki/Popliteus_muscle.
Because of the location of the origination and insertion points, when it contracts normally you bend your knee. In fact, its nickname is “the key that unlocks the knee.”
The muscle shortens and you bend your knee so you can sit down. However, you are sitting for a while and the muscle experiences muscle memory, so the muscle now “thinks” it is supposed to be shorter.
You then try to straighten your leg and stand up. However, the muscle is too short to make that movement, and it pulls hard on your knee joint. Since the muscle is so deep, you feel the pain deep inside the joint, and it may feel like a knife cutting into the back of your knee.
Treatment…
Fortunately, all you need to do is press your fingertips into the muscle, hold it for about 15 seconds, and then s-l-o-w-l-y straighten your leg. The pressure will force toxins out of the fibers, and straightening your leg will stretch the fibers.
Prevention…
When you are sitting for extended periods of time, simply stretch out your legs every 10 minutes or so. That will stretch the muscle before it has the chance for muscle memory to shorten the fibers.
What’s New For This Year?
This year I’m going to continue explaining why various muscles cause pain from the top of your head to your feet. The difference will be that I’ve already posted most of the self-treatments, and if you have one of my books, you definitely have all of the self-treatments.
Plus, there’s something exciting happening in 2024!
I’ve been working with my webmaster to start a yearly membership program where people can join and get:
*24/7 lifetime online access to my eBook: The Pain-Free Athlete
*a Perfect Ball (free shipping in the USA only),
*two 15 minute Zoom consultations where we can isolate the member’s pain situation, and
*access to several members-only group Zoom meetings over the course of the year.
This membership program will be renewable each year (sans the book and ball) so members will be able to quickly discover the source of their pain before it becomes an issue.
This book has been called “the bible” by athletes because they could find all their answers in it.
You can also have it in your home so you can Stop Pain FAST!
Watch for more new and exciting changes happening in 2024!
Wishing you well,
Julie Donnelly
www.FlexibleAthlete.com
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
About The Author
Julie Donnelly has been a licensed massage therapist since 1989, specializing in the treatment of chronic pain and sports injuries. The author of several books including Treat Yourself to Pain-Free Living, The Pain-Free Athlete, and The 15 Minute Back Pain Solution.
Julie has also developed a proven self-treatment program for the symptoms of carpal tunnel syndrome.
She has a therapy practice in Sarasota, Florida, and she travels around the USA to teach massage and physical therapists how to do the Julstro Method, and she also teaches self-treatment clinics to anyone interested in taking charge of their own health and flexibility.
She may be reached at her office: 919-886-1861, or through her website: www.FlexibleAthlete.com
Should You Follow Your Doctor’s Advice About Calcium Supplementation?
Author: Dr. Stephen Chaney
Are calcium supplements good for your heart or bad for your heart? If you don’t know the answer to that question, don’t feel badly. You have every right to be confused. Some studies say that calcium supplements increase heart disease risk while others say they decrease heart disease risk. The headlines have veered between “killer calcium” and “beneficial calcium”.
The trend appears to be moving in a positive direction. In recent years most of the studies have suggested that calcium supplements either decrease heart disease risk or have no effect on heart disease risk.
However, the medical profession has been slow to take note of this trend. Most medical societies and health professionals have focused on earlier studies and are still recommending that their patients get calcium from food rather than from supplements. I will talk more about that recommendation below.
The authors of this study performed a meta-analysis of 12 double-blinded randomized clinical trials with 87,899 participants comparing the effect of a calcium supplement versus a placebo on heart disease outcomes (heart attack, stroke, heart failure, cardiovascular mortality, and all-cause mortality).
The studies included in this analysis:
Used calcium doses from 500 mg/day to 2,000 mg/day.
Used supplements with calcium coming from a variety of sources (calcium carbonate, calcium citrate, calcium gluconolactate, and tricalcium phosphate).
Ranged from 18 months to almost 12 years in length.
Were performed with population groups from a wide range of countries (United States, England, France, Australia, New Zealand, European Union, Denmark, and Thailand).
Included calcium supplements with and without vitamin D.
Were primarily (86% of participants) conducted with post-menopausal women. One small study (0.3% of participants) was conducted with non-osteoporotic men. The rest were conducted with mixed populations (men and women) diagnosed with colorectal adenoma.
Are Calcium Supplements Heart Healthy?
This is the largest meta-analysis performed to date of double-blind, placebo-controlled randomized clinical trials on the effect of calcium supplementation versus a placebo on heart disease outcomes. This study found no effect of calcium supplementation on:
Heart attack.
Stroke
Heart failure.
Cardiovascular mortality.
All-cause mortality.
This study also evaluated potential confounding variables and found no effect of calcium supplementation on heart disease risk for:
Calcium supplements with and without vitamin D.
Dosage of calcium in the supplements (The dosage ranged from 500 mg/day to 2,000 mg/day).
Females (I suspect the number of males in this study was too small to come to a statistically significant conclusion).
Duration of calcium supplementation ≤ 5 years (The shortest duration of calcium supplementation in these studies was 18 months).
Different geographical regions.
However, this meta-analysis reported considerable variation between studies included in the analysis. Simply put,
Some studies showed an increase in heart disease risk.
Some studies showed a decrease in heart disease risk.
Some studies showed no effect on heart disease risk.
What this analysis showed was that when you combine all the studies, the aggregated data is consistent with calcium supplementation having no effect on heart disease risk.
The authors concluded, “Calcium supplementation was not associated with myocardial infraction [heart attack], stroke, heart failure, and cardiovascular/all-cause mortality. Further studies are required to examine and understand these associations.
Should You Follow Your Doctor’s Advice About Calcium Supplementation?
As I said above, most medical societies and health professionals have focused on earlier studies and are still recommending that their patients get calcium from food rather than from supplements. That may be the advice you are getting from your doctor.
Before you assume your doctor isn’t keeping up with the latest science and ignore his or her advice, we should ask why they are giving that advice. The top three reasons most medical societies give for recommending dietary sources of calcium are:
1) Some studies do show an increased risk of heart disease associated with calcium supplementation. The prime directive for health professionals is to do no harm. Yes, the average of all studies shows no effect of calcium supplementation on heart disease risk. But what if the studies showing increased risk are true for some of their patients? Those patients could be harmed.
Are you someone who might be at increased risk for heart disease if you take calcium supplements. The short answer is we don’t know because previous studies have not asked the right questions.
In my opinion, it is time to pause additional studies and meta-analyses on calcium supplementation and heart health until we have gone over existing studies with a fine-tooth comb to figure out why the results differ so wildly. For example, we need to ask whether the effect of calcium supplements on heart disease risk is influenced by things like:
Age or ethnicity of participants.
Other preexisting health conditions.
Other lifestyle factors (exercise is probably the most important, but others may be involved as well).
Diet context. For example, we already know that the effect of eggs and dairy on heart health is influenced by diet context. [I have covered this for eggs in a previous issue of “Health Tips From the Professor”.]
Other unanticipated variables.
Only when we have identified variables that might influence the effect of calcium supplements on heart disease risk, will the scientific community be able to design studies to identify the population groups who might be adversely affected by calcium supplementation.
This would allow health professionals to make informed decisions about which of their patients should avoid calcium supplementation and which of their patients would benefit from calcium supplementation.
2) We really don’t need the recommended RDAs for calcium to build strong bones. The recommended RDAs for calcium are 1,000 mg/day for adults 19-50, 1,000 mg/day for men and 1,200 mg/day for women 51-70, and 1,200 mg/day for both men and women over 70. But do we really need that amount of calcium to build healthy bones?
I have discussed this topic in detail in a previous issue of “Health Tips From the Professor”. Here are the key points:
The current RDAs are based on calcium needs for people consuming the typical American diet and following the typical American lifestyle. If that is you, the current RDAs probably apply.
However, strong bones are absolutely dependent on three things, adequate calcium, adequate vitamin D, and adequate weight-bearing exercise. Most recent studies of calcium supplementation and bone density include adequate vitamin D, but almost none of them include exercise. Previous studies have been inadequate.
The best calcium supplements contain certain nutrients besides vitamin D that optimize bone formation. I have listed those nutrients in the article cited above.
Our ability to use calcium to build strong bones is dependent on diet (something I call a bone-healthy diet) and lifestyle (something I call a bone-healthy lifestyle).
For more information on each of these points, read the article I referenced above.
In short, I agree that the current calcium RDAs may be too high for individuals consuming a bone-healthy diet and following a bone-healthy lifestyle. But the current calcium RDAs are likely accurate for people consuming the typical American diet and following the typical American lifestyle.
While we do not have a calcium RDA for populations following a bone healthy diet lifestyle, some studies suggest that 700-800 mg of calcium/day may be sufficient for this group.
3) Calcium from supplements is absorbed faster and gives higher blood level spikes than calcium from foods. That could be a problem because high blood levels of calcium are associated with calcification of our arteries, which is associated with increased heart disease risk.
This is a theoretical concern, because high blood calcium levels from supplementation are transitory, while it is continuous high blood calcium levels that are associated with calcification of our arteries.
However, it is a plausible concern because most supplement companies design their calcium supplements based on how quickly they get calcium into the bloodstream rather than how effectively the calcium is utilized for bone formation. Here are my recommendations:
Choose a calcium supplement that provides RDA levels of vitamin D plus other nutrients shown to support strong bone formation.
Choose a calcium supplement supported by clinical studies showing it is effectively utilized for bone formation.
4) We should be getting our calcium from foods rather than supplements.
While it is always easy for doctors to recommend that we get our nutrients from food rather than supplements, they need to ask whether we are getting those nutrients from our diet. For calcium the data are particularly sobering.
The average American gets around 740 mg of calcium/day from their diet. That is probably enough for the small percentage of Americans following a bone healthy diet and lifestyle. But it is 260-460 mg short of the 1,000-1,200 mg/day recommended for older adults with the typical American diet and lifestyle.
And for the average American, around 70% of their calcium intake comes from dairy foods.
So, Americans who are following a typical American diet and lifestyle and are restricting dairy may require 800-1,000 mg/day of supplemental calcium unless they carefully plan their diets to optimize calcium intake.
Finally, vegans average about 550 mg/day from their diet. That might be borderline even if they were following a bone healthy lifestyle.
In short, we cannot assume our diet will provide enough calcium for strong bones unless we include dairy foods and/or plan our diet very carefully. Some degree of supplementation may be necessary.
How Much Calcium Do You Need?
I have covered a lot of territory in this article, so let me summarize the four concerns of the medical community and answer your most important question, “Should you take calcium supplements?”
1) Calcium supplements may increase the risk of heart disease for some people.
That is true, but we have no idea at present who is at increased risk and who isn’t. So, we should minimize our risk by taking the precautions I describe below.
2) We don’t need RDA levels of calcium to build strong bones. That is probably true if you are one of the few people who follows a bone healthy diet and lifestyle, but it isn’t true if you follow the typical American diet and lifestyle.
The current RDAs of 1,000 – 1,200 mg/day are a good guideline for how much calcium you need if you follow the typical American diet and lifestyle.
If you a one of the few people who follow a bone healthy diet and lifestyle (For what that involves, read this article) you may only need 700-800 mg/day. But we don’t have clinical studies that can tell us what the actual RDA for calcium should be under those circumstances.
3) Calcium from supplements is absorbed faster and gives higher blood calcium spikes than calcium from foods. You may remember that the theoretical concern is that even short-term spikes of high blood calcium may lead to calcification of your arteries, which increases your risk of heart disease. So, the important question becomes, “What can we do to minimize these spikes in blood calcium levels?”
We should avoid calcium supplements that brag about how quickly and efficiently the calcium is absorbed. That could lead to calcium spikes. Instead, we should look for calcium supplements that are backed by clinical studies showing they are efficiently utilized for bone formation.
We should look for calcium supplements that include RDA levels of vitamin D and other nutrients that optimize bone formation. You will find more information on that in the same article I referenced above.
Some experts recommend that calcium supplements be taken between meals. But it is probably better to take them with meals because foods will likely slow the rate at which calcium is absorbed and reduce calcium spikes in the blood.
We are told to limit calcium supplements to less than 500 mg at any one time because calcium absorption becomes inefficient at higher doses. It might be even better to limit calcium to 250 mg or less at a time to reduce calcium spikes in the blood.
4) We should get calcium from foods rather than supplements.
Many Americans do not get enough calcium from diet alone, especially if they avoid dairy foods. So, some degree of calcium supplementation may be necessary. I have given some guidelines depending on your diet and lifestyle above.
The amount of supplemental calcium needed is relatively small. I do not recommend exceeding the RDA unless directed to by your health professional.
The Bottom Line
Some studies say that calcium supplements increase heart disease risk while others say they decrease heart disease risk. The headlines veer between “killer calcium” and “beneficial calcium”.
The trend appears to be moving in a positive direction. In recent years most of the studies have suggested that calcium supplements either decrease heart disease risk or have no effect on heart disease risk.
However, the medical profession has been slow to take note of this trend. Most medical societies and health professionals have focused on earlier studies and are still recommending that their patients get calcium from food rather than from supplements.
A recent meta-analysis of 12 double-blinded randomized clinical trials with 87,899 participants comparing the effect of a calcium supplement versus a placebo on heart disease outcomes has just been published. This study found no effect of calcium supplementation on:
Heart attack.
Stroke.
Heart failure.
Cardiovascular mortality.
All-cause mortality.
The authors of the study concluded, “Calcium supplementation was not associated with myocardial infraction [heart attack], stroke, heart failure, and cardiovascular/all-cause mortality.
For more details and advice on whether you should follow your doctor’s recommendations for calcium supplementation read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Why is the advice on healthy diets so confusing? One blog claims the vegan diet is best. Another says it is the keto diet is best. The Mediterranean diet is popular, but other experts claim the DASH or MIND diet might be better. Blogs champion diets ranging from the familiar to downright weird.
If you try to keep up with the science, it seems like the science is constantly changing. Each week you see headlines saying the latest study shows diet “X” is best – and “X” keeps changing. Why is that? Why do studies on healthy diets keep coming up with conflicting conclusions?
I have discussed the strengths and weaknesses of clinical studies and why they provide conflicting results in detail in previous issues of “Health Tips From the Professor”. However, one factor I have not discussed in detail is the effect of genetics on how we utilize foods, something called nutrigenomics.
Simply put, we are all genetically different. The way we utilize foods is different. The effect that foods have on our bodies is different. I have touched on that briefly in a previous article discussing individual difference in blood sugar response to various foods. But that is just one of many examples.
We do not yet know enough about gene-nutrient interactions to use genomic data to accurately predict which diets are best. Again, I have covered that topic in a previous issue of “Health Tips From the Professor”. However, we do know that genetic differences have a big influence on which diet is best for us. And most clinical studies on diets do not even attempt to take genetic differences into account.
That is where twin studies come in. Identical twins (monozygotic twins) have an identical genetic makeup and usually have an identical environment until they become adults. So, when I saw an identical twin study (MJ Landry et al, JAMA Network Open, 6(11):e2344457, 2023) comparing a vegan diet (only plant foods) with an omnivorous diet (both animal and plant foods), I wanted to review it and share it with you.
How Was The Study Done?
Identical twins were recruited from the Stanford Twin Registry. Twenty-two identical twin pairs were chosen for this study. Their characteristics were average age = 40, BMI = 26% (moderately overweight), sex = 77% female, ethnicity = 73% white, followed by an approximately equal representation of Asian, black, multiracial, and Pacific Islander.
One unanticipated characteristic of this group of twins was that 70% of them still lived together and cooked together, so their environment was also very similar.
One twin of each pair was put on a healthy vegan diet and the other on a healthy omnivorous diet for 8 weeks. Both diets were designed by dietitians. The diets emphasized fruits, vegetables, and whole grains while limiting added sugars and refined grains.
Both diets were healthier than the diets the twins were eating prior to the study. Finally, the participants were not told how much to eat, and were not instructed to lose weight.
For the first four weeks the participants were provided with all their meals by a nationwide food delivery company. The participants were also provided with training on purchasing and preparing healthy foods for their diet. This prepared them for the last 4 weeks of the study in which they purchased and prepared their own meals.
Participants visited the Stanford Clinical and Translational Science Research Unit at the beginning of the study and at the end of weeks 4 and 8 for weight measurement and a fasting blood draw.
Adherence to the diets was measured by a series of unannounced interviews to administer a 24-hour dietary recall questionnaire. These were scheduled for the weeks they visited the clinic.
What Can Twins Tell Us About Diet?
Even though the sample size was small, there were three statistically significant results.
LDL-cholesterol was reduced by 12% for the twin on the vegan diet, while it remained unchanged for the twin on the omnivorous diet.
The fasting insulin level was reduced by 21% for the twin on the vegan diet, while it remained unchanged for the twin on the omnivorous diet. This suggests the twin on the vegan diet was experiencing improved blood sugar control after just 8 weeks.
The twin on the vegan diet lost 4 pounds in 8 weeks, while weight remained the same for the twin on the omnivorous diet. This occurred even though neither twin was instructed to eat less nor to lose weight. It is most likely a consequence of the lower caloric density of the vegan diet (See my discussion of caloric density in last week’s issue of “Health Tips From the Professor”.
The changes in LDL-cholesterol and fasting insulin were remarkable because none of the twins in this study had elevated LDL-cholesterol or problems with blood sugar control at the beginning of the study.
The authors of this study concluded, “In this randomized clinical trial of the cardiometabolic effects of omnivorous vs vegan diets in identical twins, the healthy vegan diet led to improved cardiometabolic outcomes compared with a healthy omnivorous diet. Clinicians can consider this dietary approach as a healthy alternative for their patients.”
[Let me decipher the term cardiometabolic for you. The decrease in LDL-cholesterol is associated with heart health – the cardio portion of the term. The decrease in fasting insulin is associated with decreased risk of diabetes. Since diabetes is considered a metabolic disease, this is the metabolic portion of the term.]
Were There Any Downsides To The Vegan Diet?
This study also highlighted two well-known limitations of vegan diets.
Although the differences were not statistically significant, the authors expressed concern that vitamin B12 intake was less for twins on the vegan diet than twins on the omnivorous diet even though the vegan diet was designed by dietitians.
The authors noted that B12 deficiency among vegans is well known, and said, “Long-term vegans are typically encouraged to take a cyanocobalamin (vitamin B12) supplement.
Although both groups had excellent adherence to their assigned diets, those assigned to the vegan diet expressed a lower satisfaction with the diet, which suggests long-term adherence to the diet after the study ended was unlikely.
The authors said, “Although our findings suggest that vegan diets offer a protective cardiometabolic advantage compared with a healthy omnivorous diet, excluding all meats and/or dairy products may not be necessary because research suggests that cardiometabolic benefits can be achieved with modest reduction in animal foods and increases in healthy plant-based foods compared with typical diets.”
“We believe that lower dietary satisfaction in the vegan group may have been attributable to the strictness of the vegan diet…Some people may find a less restrictive diet preferable for LDL-cholesterol-lowering effects.”
I concur.
What Are The Pros And Cons Of Twin Studies?
The Pros are obvious. Most dietary studies cannot take genetic differences into account and have difficulty accounting for environmental differences. In this study genetics was identical for each twin pair and their environment was very similar. It offers a unique advantage over other studies.
But the strength of this study is also its greatest weakness. Because the general population is genetically and environmentally diverse, it is difficult to extrapolate the results to the general population.
If this were the only study to show cardiometabolic benefits of a plant-based diet, it would simply be an interesting observation.
But there are several studies showing that the vegan diet is associated with lower weight and reduced risk of heart disease and diabetes.
And there are dozens of studies showing that primarily plant-based omnivorous diets reduce the risk of heart disease and diabetes.
This study is fully consistent with those studies.
The Bottom Line
A recent study put identical twins on either a healthy vegan diet (only plant foods) or a healthy omnivorous diet (both animal and plant foods) for 8 weeks. At the end of 8 weeks:
LDL-cholesterol was reduced by 12% for the twin on the vegan diet, while it remained unchanged for the twin on the omnivorous diet.
The fasting insulin level was reduced by 21% for the twin on the vegan diet, while it remained unchanged for the twin on the omnivorous diet. This suggests the twin on the vegan diet was experiencing improved blood sugar control after just 8 weeks.
The twin on the vegan diet lost 4 pounds in 8 weeks, while weight remained the same for the twin on the omnivorous diet. This occurred even though neither twin was instructed to eat less or to lose weight. It is most likely a consequence of the lower caloric density of the vegan diet.
The changes in LDL-cholesterol and fasting insulin were remarkable because none of the twins in this study had elevated LDL-cholesterol or problems with blood sugar control at the beginning of the study.
The authors of this study concluded, “In this randomized clinical trial of the cardiometabolic effects of omnivorous vs vegan diets in identical twins, the healthy vegan diet led to improved cardiometabolic outcomes compared with a healthy omnivorous diet. Clinicians can consider this dietary approach as a healthy alternative for their patients.”
For more information on the pros and cons of this study and what it means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
For the past 35 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
You are probably tired of hearing about how bad processed foods are for you. If you have been following the headlines, you probably already know that diets high in processed foods are linked to obesity, type 2 diabetes, heart disease, some forms of cancer, memory loss, liver disease, kidney disease, depression, risk of dying from any cause, and much more.
And this is a serious problem because 60-70% of the American diet comes from processed foods.
In fact, you may have seen these headlines so frequently that your eyes glaze over, and your mind shuts down any time you see the words “processed foods” in the title.
This week I will be sharing the latest studies on why processed foods make us fat. Stick with me on this. This is not just another article on processed foods. While the focus of the article is on processed foods, the studies it covers are valuable because they also identify some unprocessed foods that can make us fat.
Spoiler alert! Today’s “Health Tip” is important because it teaches us that weight control is not as simple as eliminating processed foods from our diet. We also need to know which unprocessed or minimally processed foods to eat less of.
Before I proceed, I should give you a brief review of how processed foods are defined because that definition has changed in recent years.
What Are Processed Foods?
Everyone used to have a good understanding of which foods were processed. But several years ago, the scientific community introduced a new food classification system called “The NOVA food classification system” and introduced a new category – ultra-processed foods. I have covered this classification system in previous “Health Tips From the Professor” articles, but I will review it here.
The NOVA system categorizes foods into four groups according to the extent of processing they have undergone:
Unprocessed foods.
This category includes foods like fruit, vegetables, milk, eggs, and meat.
2) Processed culinary ingredients.
This category includes foods you might find in restaurants or prepare yourself to which things like salt, sugar, vegetable oils, butter, or cream were added in the preparation.
3) Minimally processed foods.
This category includes foods like canned vegetables, freshly made breads, and cheeses.
4) Ultra-processed foods.
This category includes foods like soft drinks, chips, packaged snacks, most breakfast cereals, chicken nuggets & fish sticks, fast food burgers, hot dogs, and other processed meats.
The actual list is much longer, but you get the idea. What we call processed foods, scientists now call ultra-processed foods. The article I am discussing used the term “ultra-processed foods” in the title.
But, since the term “ultra-processed foods” has not yet entered the popular vocabulary, I will use the term “processed foods” in this article because it is more understandable to the average reader.
Does Processed Food Make You Fat?
I shared a study in a previous issue of “Health Tips From the Professor” that suggested that the answer was yes, but did not answer the question of why. That’s because of the way the experiment was designed.
The ultra-processed diet and unprocessed diets were matched with respect to:
Total calories in the food portions given to the subjects.
Caloric density (calories per serving size). That’s because caloric density has been linked to overeating (I’ll discuss that in more detail below.) The authors of the study eliminated that variable.
Macronutrients (carbohydrate, fat, & protein). I’m sure you’ve seen blogs suggesting that carbohydrates or fat cause weight gain. And you’ve probably seen blogs suggesting that high protein diets cause weight loss. The authors eliminated these variables.
Total sugar, fiber, and sodium. That’s because the sugar, fat, and sodium content of foods increase their tastiness (palatability), which has been linked to overeating (more below). The authors eliminated this variable.
In short, this study compared a tasty, healthy ultra-processed food diet with a tasty, healthy unprocessed food diet. [Note: This does not represent the real world. In the real world the ultra-processed foods eaten by most Americans are higher in caloric density, sugar, fat, and sodium and lower in fiber than unprocessed foods.]
However, in the scientific world, this was an excellent study design. By eliminating variables thought to explain the correlation between ultra-processed food consumption and obesity, the study was able to focus on two questions:
#1: With those variables eliminated, do ultra-processed foods still lead to overeating?Here the answer was a clear, yes.
The study participants eating ultra-processed foods ate 500 more calories per day than those eating unprocessed foods. (Both groups were presented with meals and snacks containing the same number of calories and told to eat as much as they wanted.)
Participants eating ultra-processed foods gained 2 pounds in just two weeks, while those eating unprocessed foods lost 2 pounds.
#2: If so, what else about ultra-processed foods leads to overeating? One popular theory of why ultra-processed foods lead to overeating is that they cause large blood sugar spikes and crashes, which stimulates appetite. But the authors of the study were disappointed to find no large blood sugar spikes following consumption of ultra-processed food meals.
However, I don’t think their data disproves the blood sugar spike theory. Remember that this was a “healthy ultra-processed food diet”. The amount of sugar and fiber was identical in the ultra-processed and unprocessed food diets. More importantly, when I looked at the sample menus provided by authors as supplementary information, each meal contained a significant percent of whole, low-glycemic foods. This was a “healthy ultra-processed food” diet designed by a dietitian, not what the typical American eats.
So, why did the ultra-processed food group eat more in this study? This study did not provide an answer to that question, but other studies (described below) have provided probable answers to that question.
Why Does Processed Food Make You Fat?
What do other studies tell us about why processed foods make us overeat and gain weight? Here are the top 7 mechanisms that have been suggested and what they mean for us.
#1: Caloric Density: Simply put, caloric density is the number of calories in a serving of food. When you consume foods with a high caloric density, you are more likely to consume excess calories without even thinking about it.
When I was still teaching medical students, I used this example to illustrate the effect of caloric density on calories consumed. “There are the same number of calories in a 2-ounce candy bar and a pound of apples. You can eat a 2-ounce candy bar and be ready to eat more. If you eat a pound of apples, you are done for a while”.
Since most processed foods have a higher caloric density than unprocessed foods, the simplest solution to weight control is to limit processed foods in your diet.
However, how you or your favorite restaurant prepares unprocessed foods is important as well. For example, the addition of cheese or cream sauces can significantly increase the caloric density of the food. This is why the NOVA food classification system I described above created a new category of “culinary foods” to describe these kinds of foods.
#2: Hyper-palatability: In prehistoric times foods that were sweet, salty, and fatty were essential for survival, so we are hardwired to desire those foods. Here is why:
We need a certain amount of sugar for our brain, red blood cells, and a few other tissues to function. Wild game provides almost no carbohydrate. Fruits were the best source of sugar, but fruits were scarce prior to farming. The craving for sweetness drove us to forage far and wide to find fruits and other plant sources of sugar and carbohydrate.
Sodium is essential for survival, but unprocessed plant and animal foods provide very little. That’s why even in Biblical times, salt was worth its weight in gold.
In prehistoric times, food was sometimes scarce, especially in winter. It might be a week or more between meals. Fat stores got prehistoric man through these times of scarcity, so it was important to eat fatty meals in times of plenty. [Note: We no longer live in times of scarcity, and those fat stores have gone from being an asset to being a health concern.]
Unfortunately, “Big Food, Inc” has weaponized these hardwired desires for sweet, salty, and fatty foods. Simply put, processed foods taste good because they fulfil our hardwired taste desires. Scientists call it “hyper-palatability”. But whatever you call it, we want to eat more, and that leads to overeating.
And again, the way we prepare the foods we eat also matters. It’s only natural to add extra salt, sugar, and/or fat to the foods we prepare so they taste better. And if we add too much, we make the healthy foods we eat hyper-palatable, and we are tempted to overeat.
On a personal note, I never knew you might want to add sugar and fat to the vegetables you cook before my family moved to the south. On the other hand, I had never eaten collard greens before either.
#3: Food Consistency: When you look at studies on the effect of food consistency on calories consumed, you find that there are several different ways of defining food consistency, but they are all looking at the same thing from a different perspective – like the fable of the 6 blind men trying to describe an elephant.
applesauce
Food Structure: The classic study, published in 2009, compared the effect of sliced apples, applesauce, and apple juice eaten shortly before a meal on the number of calories consumed at the meal. In terms of calories consumed during the meal, the results were clear. It was apple juice > applesauce > apple slices.
This drew attention to the effect of food structure on calories consumed. Apples are a whole food with cellular structure intact. Applesauce contains all the nutrients, phytonutrients, and fiber of whole apples, but the cellular structure has been lost. Apple juice contains most of the nutrients and phytonutrients of applesauce, but the fiber has been lost.
Why does the structure of whole foods matter?
Cell structure must be destroyed before digestion can occur, the release of sugar and carbohydrates from the food is delayed. This reduces the spikes and valleys of blood sugar that can increase appetite.
Transit time of the food through the intestine is also delayed. Thus, the feeling of fulness persists longer, which reduces appetite.
There are two takeaway lessons from this study that may not be so obvious:
Neither applesauce nor apple juice meet the NOVA definition of an ultra-processed food. So, simply removing processed foods from your diet may not be enough to reduce your appetite and, therefore, your caloric intake.
In addition, adding fiber back to apple juice did not make it equivalent to applesauce in reducing appetite. So, despite what Big Food Inc tells you, adding fiber to processed foods does not turn them into health foods.
Soft Versus Hard Foods:Many processed foods are soft, and most unprocessed foods are hard. So, you could think of this as a description that separates processed foods from unprocessed foods.
But, if you consider the apples versus applesauce comparison I described above, it is obvious that soft versus hard description also pertains to minimally processed foods such as applesauce and whole, unprocessed foods such as apples.
For example, one recent study comparing soft versus hard foods found it didn’t matter whether the soft foods were processed or unprocessed. People in the study ate more calories from all soft foods than from hard, unprocessed foods such as raw fruits and vegetables.
Fast Versus Slow Foods:This description separates foods based on the speed at which they are digested and pass through the intestine. Once again, you might think of this as a description that separates processed and unprocessed foods until you think about applesauce versus apples comparison.
And, as you might expect, a recent study comparing “fast” versus “slow” foods found it didn’t matter whether the fast and slow foods were processed or unprocessed. People in the study ate more calories from fast foods than from slow foods.
[Note: This study defined “slow” foods as harder, chunkier, more solid, and more viscous. While the first three adjectives describe what other scientists also refer to as “hard” foods, the final adjective broadens the category to include “soft” foods like oatmeal.]
How Can You Enjoy Eating Without Getting Fat?
For most Americans, weight is a constant uphill battle. Their weight increases by a few pounds every year, and over time that continuing weight gain adds up. Diets are never enjoyable, which is part of the reason they almost always fail in the long term. You want to control your weight, but you also want to enjoy what you eat. Why is that so hard?
The secret to a healthy weight is to find foods you enjoy that don’t increase your appetite – foods that fill you up, so you eat less naturally. Here are my 4 tips for eating foods you enjoy without getting fat.
Tip #1: Limit processed foods. Processed foods tend to have a high caloric density; are hyper-palatable, soft, and fast; and lack the intact cellular structure of whole, unprocessed foods. And multiple studies, such as the one I cited above, agree that processed foods cause us to eat more and to gain weight. So, the single most important step you can take to control your weight is to limit your intake of processed foods.
Tip #2: Choose minimally processed foods wisely. The studies I shared above suggest that avoiding processed foods may not be enough. We also need to look at the minimally processed foods we eat (applesauce, for example). These studies suggest we should also favor whole, unprocessed foods over minimally processed foods that are softer and faster (more quickly digested).
By now, you might be saying, “Wait a minute. I thought you said I could enjoy eating without getting fat. How can I enjoy eating if I have to give up my favorite processed and minimally processed foods?”
My short answer would be, “No. But you might want to broaden your horizons”. We all tend to be creatures of habit. We eat a relatively small variety of foods on a regular basis. When my wife and I decided to eat healthier, we kept trying new foods until we found new, healthier foods we loved.
The category of whole unprocessed foods offers many options. There are fruits, vegetables, many varieties of 100% whole grains, beans, nus, seeds, eggs, and meats. And we are blessed to live in a country with abundant choices. When you walk into your local supermarket you will find dozens of foods in each of these categories that you have never tried before. Be daring. Keep trying new foods until you find new favorite foods you love.
Tip #3: Be aware of how foods are prepared. The studies described above also suggest how we prepare the food is important. We can start out with a whole unprocessed food and end up with something no better than processed food if we prepare it incorrectly. If we add lots of cream, cheese, butter, and/or sugar, we increase the caloric density. And this can lead to us consuming more calories without even thinking about it.Throw in some salt and we have also made the food hyper-palatable, which makes us want to eat more.
Now you might be saying, “But I grew up with my food being cooked this way. This is my comfort zone. Do I have to completely change the way I cook my food, and the items I choose at my favorite restaurant?”
Again, my short answer would be, “No, but you might want to try new recipes.” I am not a cooking guru. That would be my wife. But I do know there are lots of books and web sites featuring healthy recipes. Once again, be bold. Try new recipes until you find new favorites. Try new items on your favorite restaurant’s menu or try new restaurants until you find healthier, restaurant foods you love.
Tip #4: Never say never. This is perhaps the most important tip. Whenever we tell ourselves we can never eat a food again, it becomes irresistible. We are setting ourselves up for failure. The goal should be to change unhealthy foods and unhealthy recipes from an everyday occurrence to an occasional pleasure.
The Bottom Line
Multiple studies show that eating processed foods leads to weight gain. It may be no coincidence that 60-70% of the foods Americans eat is highly processed and 60-70% of us are overweight or obese.
In the article above, I summarize recent studies asking why processed foods make us fat. If you think these studies are only of interest to scientists, you would be wrong. These studies also help us to identify unprocessed and minimally processed foods in our diet that can make us fat.
For more information on these studies, and 4 tips on how you can enjoy eating without getting fat, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Author: Julie Donnelly, LMT – The Pain Relief Expert
Editor: Dr. Steve Chaney
I hope that 2023 was kind to you and your family. Covid seemed to come and go, with new strains popping up every time we turned around. And then there is RSV and the flu. What a year!
In December the foods all seemed to be fattening – delicious for sure, but fattening. Which brings me to the topic of the month. Maybe you are trying to walk off some of the extra calories you put on last month.
Walking will help burn calories, but it can also come with aches and pains from muscles getting used repetitively.
This month I want to focus on pain that prevents you from bending your knee after several days of walking more than your body is used to. It can reduce your walks to a slow hobble at best. And that isn’t going to burn off any extra calories.
One Quadricep Muscle is the Source of Pain from the Low Back to the Knee.
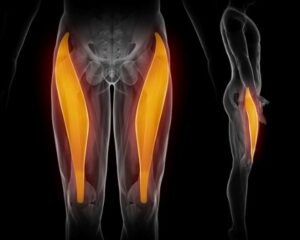
You likely already know that there are four quadriceps that form the front of your thigh. You probably also know that they are responsible for straightening your leg when you want to stand up from sitting. But there is so much more…especially for one of the quads…the rectus femoris.
Your Rectus Femoris Muscle And Knee Pain
The rectus femoris is a long muscle located in the front, and a bit toward the outside of your thigh.
The rectus femoris is the only one of the four quads that originate on the tip of your pelvis (ASIS), the rest: vastus lateralis, vastus intermedius, and vastus medialis, all originate along your thigh bone (femur). These four muscles join together and attach to your kneecap (patella).
This picture shows the muscle but fails to show the tendon that starts at the top of your kneecap, goes over your kneecap (patella), and inserts into the front of your shin bone (tibia).
It is the patella tendon that causes knee pain and can prevent you from bending your knee when you sit down or want to walk up steps.
Think of the analogy I use so frequently. When you pull your hair, your head hurts, but you don’t need to rub your head, take pain pills, or have brain surgery. You just need to let go of your hair!
In the same way, the muscle is pulling down on the front of your hip and may cause anterior hip pain, and it’s pulling up on your patella tendon, causing your kneecap to move up so you can’t bend your knee, and putting stress on your shin bone.
Your knee and front of your hip are NOT the problem, they are the symptom!
The Function Of The Rectus Femoris Muscle:
Since the muscle originates on the tip of your pelvis,
The rectus femoris flexes (bends) the hip along with two other muscles I’ve discussed in the past, the sartorius and iliopsoas. The four quads pull up on your lower leg at the knee, straightening your leg so you can stand up.
Injury To The Rectus Femoris Muscle:
In acute rectus femoris muscle injuries, a person may feel a tearing sensation at their knee, with an abrupt onset of pain.
Subacute injuries may present with gradual onset of pain at either the front of your hip or your knee. If you enjoy running, you may also have knee pain while you’re running uphill.
You may feel that you have arthritis in your knee joint. If that is the case, it is beneficial to see a deep muscle massage therapist to eliminate tight muscles from the diagnosis. You can also do the Julstro self-treatment that is shown below to release the tension in the muscle.
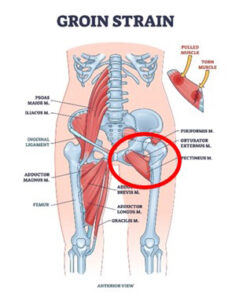
When a muscular strain injury occurs, a person may also have moderate to severe pain in the groin.
Pain can be sudden, like kicking the ball in soccer or sprinting from a standing position. Or it may build up gradually as an overuse problem with repeated tearing and repeated stress.
Stretching, without first releasing the tension in the muscle, can cause tearing where the muscle inserts into the tendon, or tear the tendon fibers from the bone.
Spasms in your rectus femoris can also be caused by contractions in the muscles that impact your lower back and pelvis. If this is the case, you need to treat each of the muscles before your thigh muscles release. I demonstrate the full treatment in my books in the chapter about the Julstro Protocol.
Treating Your Rectus Femoris Muscle Safely
There are multiple ways to treat your rectus femoris muscle and I show them to you in my books: The Pain-Free Athlete and Treat Yourself to Pain-Free Living.
Using a 12” length of 1” PVC pipe, place the pipe as shown in this picture. This is the perfect position to treat the rectus femoris.
Hold the pipe loosely in your hand or hold your four fingers straight out so you are not curling them around the pipe. This will prevent tension from forming in your forearm muscles.
Press into your thigh and slide, don’t roll, down your thigh to just above your knee.
Do this to your entire thigh, outside/front/inside so you treat all four quadriceps.
I suggest you treat both thighs, even if you are only having pain in one leg.
Wishing you well,
Julie Donnelly
www.FlexibleAthlete.com
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
About The Author
Julie Donnelly has been a licensed massage therapist since 1989, specializing in the treatment of chronic pain and sports injuries. The author of several books including Treat Yourself to Pain-Free Living, The Pain-Free Athlete, and The 15 Minute Back Pain Solution.
Julie has also developed a proven self-treatment program for the symptoms of carpal tunnel syndrome.
She has a therapy practice in Sarasota, Florida, and she travels around the USA to teach massage and physical therapists how to do the Julstro Method, and she also teaches self-treatment clinics to anyone interested in taking charge of their own health and flexibility.
She may be reached at her office: 919-886-1861, or through her website: www.FlexibleAthlete.com
Weight gain during pregnancy is a challenge for many women. The Centers for Disease Control has stated that 48% of women gained more than the recommended amount of weight during pregnancy, only one third (32%) of women gained the recommended amount and 21% of women gained too little[i]
Weight is a big thing to be concerned about and to work on prior to and during pregnancy. Why do you need to worry about this? One’s weight prior to pregnancy can make it more difficult to become pregnant. And weight gain during pregnancy carries lifelong implications for both the mother and infant.
Many women think that during pregnancy, that they must “Eat for Two”, thus giving them the feeling that they should eat more to nourish a developing baby. However, this saying needs to be re-examined, as I explain below.
Nutrition during pregnancy is really, really important. It lays down the physical foundation for your baby and has lifelong implications for both mother and baby. Keep in mind, you are growing a baby!
So how much weight should I gain during pregnancy? Weight gain in pregnancy will be based upon your body mass index or BMI.
What is the body mass index? The Body mass index (BMI) is a measure of body fat based on height and weight that applies to adult men and women. A calculator is used to determine your BMI. [ii] Calculators to measure BMI can be downloaded from the Apple store and Google Play.
It is going to be the determining factor for how much weight you should gain during pregnancy.
So, Based On Your BMI, How Much Weight Should You Gain During Pregnancy?
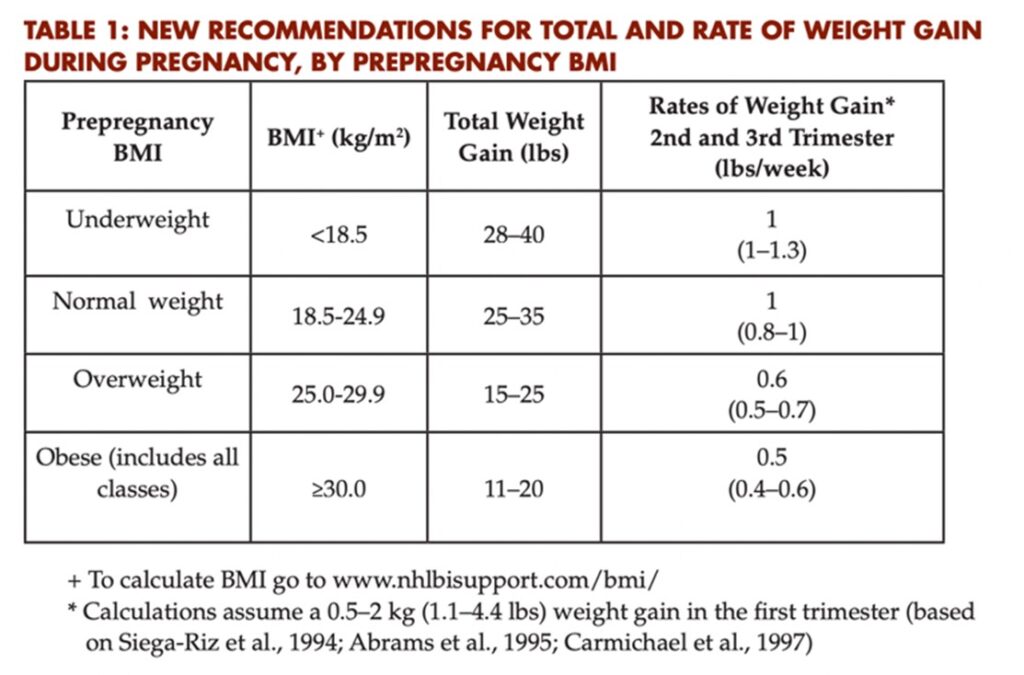
The Institute of Medicine recommends that, based upon your pre-pregnancy BMI, weight gain during pregnancy can range from zero pounds up to 40 pounds during pregnancy.
If you are underweight, weight gain between 28 and 40 pounds is recommended.
If you are at normal weight, the recommended weight gain is between 25 to 35 pounds.
If you are overweight, the recommended weight gain is 15 to 25 pounds.
And if you are obese, the weight gain is 11 to 20 pounds during your pregnancy.[i]
Recent recommendations have proposed that obesity should be broken into three different categories. BMI 1, BMI 2 and BMI 3, and that total weight gain should be limited to zero to 15 pounds gain based on these BMI categories.[ii] Research is ongoing on these recommendations.
Proposed Weight Gain Recommendations for Pregnant Women with Obesity†
BMI Category
Current IOM Recommendations (lbs)
Proposed Recommendations (lbs)
BMI 1 (30-34.9)
11-20
5-15
BMI 2 (35-39.9)
11-20
<10
BMI 3 (≥ 40)
11-20
Maintain prepregnancy weight
J. Clin. Invest. 2019 129: 4567-4569
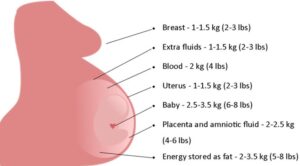
Where Does The Weight Go During Pregnancy?
Your baby and changes in your body during pregnancy account for the 25 to 35 pounds weight gain during pregnancy.
Baby – 6-8 pounds.
Placenta and surrounding water – 4-6 pounds.
Uterus – 2-3 pounds.
Enlarged breast tissue – 2-3 pounds.
Increased blood (blood volume increases 40% to 50% during pregnancy) – 4 pounds.
Fluids in the maternal tissue throughout your body – 2-3 pounds.
Fat stores – 5-8 pounds.
How Many Calories Should You Eat Each Day?
During the first trimester, it is recommended that women gain no more than four pounds. In the second and third trimesters of pregnancy, it is recommended that women should gain between one half pound to one pound per week[i].
One pound is equal to 3,500 calories. This equals to 500 calories per day which is equal to a sandwich and a glass of milk. This is definitely not “eating for two”. If you are carrying twins or triplets, this amount will increase.
What Happens If You Are Underweight Or Overweight?
Having a longer labor which can result in postpartum hemorrhage.
Increased possibility of needing to use internal monitors as external monitors cannot pick up fetal heart tone due to fat density.
Increased risk of cesarean section.
Increased risk of shoulder dystocia because the baby is also big.
Weight stays on after pregnancy, which increases the risk of overweight and obesity.
Increased risk of developing diabetes later in life.
Increased risk of repeat cesarean section.
Baby:
Increased risk of neural tube defects.
Increased risk of heart defects.
Baby is too big for weeks of pregnancy (gestational age baby).
Hyperglycemia, meaning that the baby’s blood sugar is too high.
Possibility of trauma when the baby is being born.
Long-term obesity for that child resulting in childhood obesity.
Daughters that are large for gestational age are more likely to be obese and deliver larger babies.
Underweight
Mother:
Difficulty with getting pregnant.
Increased risk of having a pre-term birth (your baby is born before 37 weeks of pregnancy).
Baby:
Increased risk for prematurity.
Increased risk that baby is small for gestational age or low birth weight.
Problems with oxygen levels at birth.
Trouble staying warm because the baby doesn’t have the fat stores that give the calories to help the baby to stay warm.
Breathing problems.
Increased problems with infection.
Nervous system problems with possible long-term effects of cerebral palsy, blindness, developmental delays where your baby is not developing on time.
What Resources Are Available To Help You Gain The Appropriate Amount Of Weight During Pregnancy?
There are many resources available, including weight gain trackers.[i] It would be wise to seek the help of a registered dietitian. If you are underweight or obese, their services may be covered under your health insurance.
The Bottom Line
Women who are overweight or underweight prior to pregnancy can have difficulty becoming pregnant.
Many women carry the idea that during pregnancy, that they are “Eating for Two”. This idea can lead to excessive weight gain for the mother that persists after pregnancy and childhood obesity for the infant.
Weight gain during pregnancy is determined by one’s pre-pregnancy body mass index (BMI).
Based upon the prepregnant BMI, weight gain during pregnancy can range from 11 pounds to 40 pounds during pregnancy. Ongoing studies are suggesting a weight gain amount of zero to 15 pounds for Obesity Categories I through III.
It is recommended that during pregnancy, mothers gain up to a total of four pounds in the first trimester and between one half to one pound per week in the second and third trimesters. This amount of weight gain equals to an additional 500 calories per day which is equal to a sandwich and one glass of whole milk additionally per day.
Weight gain during pregnancy carries lifelong implications for both mother and infant.
Seek help from a registered dietitian if you are overweight or underweight. Weight gain trackers are also available for mothers to track their weight during pregnancy at the Centers for Disease Control website.[ii]
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
About The Author
Carolyn Curtis, MSN, CNM, RN, FACNM, FAAN, has:
More than 40 years’ experience in the oversight of domestic and international programs and the provision of nursing and midwifery integrated service delivery in maternal child health, family planning, reproductive and women’s health care.
Twenty years’ experience in teaching, mentoring, and providing clinical oversight to undergraduate and graduate public health, medical, nursing and midwifery students.
The top 3 claims the advocates of every popular diet make are:
It will help you lose weight.
It reduces your risk of diabetes.
It reduces your risk of heart disease.
The truth is any restrictive diet helps you lose weight. And when you lose weight, you improve blood sugar control. Which, of course, reduces your risk of developing diabetes.
But what about heart disease? Which diets are heart healthy? When it comes to heart disease the claims of diet advocates are often misleading. That’s because the studies these advocates use to support their claims are often poor quality studies. Many of these studies:
Look at markers of heart disease risk rather than heart disease outcomes. Markers like LDL cholesterol, triglycerides, c-reactive protein, etc. are only able to predict possible heart disease outcomes. To really know which diets are heart healthy you have to measure actual heart disease outcomes such as heart attacks, stroke, and cardiovascular deaths.
Are too short to provide meaningful results. Many of these studies last only a few weeks. You need much longer to measure heart disease outcomes.
Are too small to provide statistically significant results. You need thousands of subjects to be sure the results you are seeing are statistically significant.
Have not been confirmed by other studies. The Dr. Strangeloves of the world like to “cherry pick” the studies that support the effectiveness of their favorite diet. Objective scientists know that any individual study can be wrong. So, they look for consensus conclusions from multiple studies.
A recent study (G Karam et al, British Medical Journal, 380: e072003, 2023) avoided all those pitfalls. The investigators conducted a meta-analysis of 40 high-quality clinical studies with 35,548 participants to answer the question, “Which diets are heart healthy?”
How Was The Study Done?
The authors started by searching all major databases of clinical studies for studies published on the effect of diets on heart disease outcomes through September 2021.
They then performed a meta-analysis of the data from all studies that:
Compared the effect of a particular diet to minimal dietary intervention (defined as not receiving any advice or receiving dietary information such as brochures or brief advice from their clinician with little or no follow-up).
Looked at heart disease outcomes such as all cause mortality, cardiovascular mortality, non-fatal heart attacks, stroke, and others.
Lasted for at least 9 months (average duration = 3 years).
Were high-quality studies.
Using these criteria:
They identified 40 studies with 35,548 participants for inclusion in their meta-analysis.
From those 40 studies, they identified 7 diet types that met their inclusion criteria (low fat (18 studies), Mediterranean (12 studies), very low fat (6 studies), modified fat (substituting healthy fats for unhealthy fats rather than decreasing fats, 4 studies), combined low fat and low sodium (3 studies), Ornish (3 studies), Pritikin (1 study).
One weakness of meta-analyses is that the design of the studies included in the meta-analysis is often different. Sometimes they don’t fit together well. So, while the individual studies are high-quality, a combination of all the studies can lead to a conclusion that is low quality or moderate quality.
Finally, the data were corrected for confounding factors such as obesity, exercise, smoking, and medication use.
Which Diets Are Heart Healthy?
Now that you understand the study design, we are ready to answer the question, “Which diets are heart healthy?” Here is what this study found:
Compared to minimal intervention,
The Mediterranean diet decreased all cause mortality by 28%, cardiovascular mortality by 45%, stroke by 35%, and non-fatal heart attacks by 52%.
Low fat diets decreased all cause mortality by 16% and non-fatal heart attacks by 23%. The effect of low fat diets on cardiovascular mortality and stroke was not statistically significant in this meta-analysis.
For both the Mediterranean and low fat diets, the heart health benefits were significantly better for patients who were at high risk of heart disease upon entry into the study.
The evidence supporting the heart health benefits for both diets was considered moderate quality evidence for this meta-analysis. [Remember that the quality of any conclusion in a meta-analysis is based on both the quality of evidence of the individual studies plus how well the studies fit together in the meta-analysis.]
While the percentage of risk reduction appears to be different for the Mediterranean and low fat diets, the effect of the two diets on heart health was not considered significantly different in this study.
The other 5 diets provided little, or no benefit, compared to the minimal intervention control based on low to moderate quality evidence.
The authors concluded, “This network meta-analysis found that Mediterranean and low fat dietary programs probably reduce the risk of mortality and non-fatal myocardial infarction [heart attacks] in people at increased cardiovascular risk. Mediterranean dietary programs are also likely to reduce the risk of stroke. Generally, other dietary programs were not superior to minimal intervention.”
Which Diet Is Best For You?
The fact that this study found both the Mediterranean diet and low fat diets to be heart healthy is not surprising. Numerous individual studies have found these diets to be heart healthy. So, it is not surprising when the individual studies were combined in a meta-analysis, the meta-analysis also concluded they were heart healthy. However, there are two important points I would like to make.
The diets used in these studies were designed by trained dietitians. That means the low fat studies did not use Big Food, Inc’s version of the low fat diet in which fatty foods are replaced with highly processed foods. In these studies, fatty foods were most likely replaced with whole or minimally processed foods from all 5 food groups.
The Mediterranean diet is probably the most studied of current popular diets. From these studies we know the Mediterranean diet improves brain health, gut health, and reduces cancer risk.
As for the other 5 diets (very low fat, modified fat, low fat and low sodium, Ornish, and Pritikin), I would say the jury is out. There is some evidence that these diets may be heart healthy. But very few of these studies were good enough to be included in this meta-analysis. Clearly, more high-quality studies are needed.
Finally, you might be wondering why other popular diets such as paleo, low carb, and very low carb (Atkins, keto, and others) were left out of this analysis. All I can say is that it wasn’t by design.
The authors did not select the 7 diets described in this study and then search for studies testing their effectiveness. They searched for all studies describing the effect of diets on heart health. Once they identified 40 high-quality studies, they grouped the diets into 7 diet categories.
I can only conclude there were no high-quality studies of paleo, low carb, or very low carb diets that met the criteria for inclusion in this meta-analysis. The criteria were:
The effect of diet on heart health must be compared to a control group that received no or minimal dietary advice.
The study must measure heart disease outcomes such as all cause mortality, cardiovascular mortality, non-fatal heart attacks, and stroke.
The study must last at least 9 months.
The study must be high-quality.
Until these kinds of studies are done, we have no idea whether these diets are heart healthy or not.
So, what’s the takeaway for you? Which diet is best for you? Both low fat diets and the Mediterranean diet are heart healthy provided the low fat diet consists of primarily whole or minimally processed foods. Which of these two diets is best for you depends on your food preferences.
The Bottom Line
Many of you may have been warned by your doctor that your heart health is not what it should be. Others may be concerned because you have a family history of heart disease. You want to know which diets are heart healthy.
Fortunately, a recent study answered that question. The authors performed a meta-analysis of 40 high-quality studies that compared the effect of various diets with the effect of minimal dietary intervention (doctors’ advice or diet brochure) on heart disease outcomes.
From this study they concluded that both low fat diets and the Mediterranean diet probably reduce mortality and the risk of non-fatal heart attacks, and that the Mediterranean diet likely reduces stroke risk.
Other diets studied had no significant effect on heart health in this study. That does not necessarily mean they are ineffective. But it does mean that more high-quality studies are needed before we can evaluate their effect on heart health.
So, what’s the bottom line for you? Both low fat diets and the Mediterranean diet are heart healthy provided the low fat diet consists of primarily whole or minimally processed foods Which of these two diets is best for you depends on your food preferences.
For more information on this study, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Do omega-3s reduce cognitive decline, or is this another nutrition myth?
There is certainly good reason to believe that the long chain omega-3s EPA and DHA are good for brain health.
DHA is an essential part of the membrane that coats our neurons. As such, it is a major component of our brains and plays an important role in its structural integrity.
While EPA is not found in the brain it reduces inflammation and improves blood flow to the brain, both of which are important for brain health.
But the role of DHA and EPA in reducing cognitive decline remains controversial. Some studies strongly support their role in slowing cognitive decline while other studies find no effect.
So, the question remains, “Do omega-3s reduce cognitive decline or not?”
This study supports the hypothesis that omega-3s, especially DHA and EPA, reduce cognitive decline and Alzheimer’s disease. But it also raises several questions that need to be resolved by future studies.
Why Is The Effect Of Omega-3s On Cognitive Decline Controversial?
Why is it so difficult to come up with definitive answers about whether omega-3s reduce cognitive decline? It is probably because the relationship between omega-3s and brain health is complex. For example:
Because omega-3’s beneficial effects are widely publicized, many people are already consuming adequate amounts of omega-3s. A supplement study that does not measure the omega-3 status of participants at the beginning of the study and does not focus on participants with inadequate omega-3 status is doomed to failure.
Omega-3s may benefit older people more than younger people. A study that is not large enough to measure the effect of omega-3s on both groups is doomed to failure.
The APOE ɛ4 genotype is associated with an increased risk of cognitive decline and Alzheimer’s. Some studies suggest omega-3s are more beneficial for people with the APOE ɛ4 genotype, while other studies come to the opposite conclusion. This is a critical variable that needs to be resolved.
The ability of DHA to cross the blood-brain barrier and accumulate in our brain may be influenced by our genetics, especially our APOE ɛ4 status, and adequate levels of other nutrients, especially B vitamins. Unless studies are large enough to separate out these variables, they are doomed to failure. This study suggests accumulation of DHA in the brain is a critical variable that needs to be resolved.
Multiple studies suggest that higher doses of omega-3s are more effective at reducing cognitive decline than low doses of omega-3s. This study confirms that effect and identifies a threshold dose that is needed to provide measurable benefits. Studies providing supplemental omega-3s at doses below that threshold are likely to fail. And meta-analyses that combine low dose studies with high dose studies are also likely to come up empty.
Finally, people who take omega-3s for years are likely to benefit more than those who take omega-3s for just a few months. Again, this study confirms that effect, which means that studies involving short-term supplementation with omega-3s are likely to fail. And meta-analyses that combine short-term and long-term studies are likely to come up empty.
With so many potential pitfalls, it is easy to understand why many studies come up empty, and the effect of omega-3s on cognitive decline remains controversial.
How Was This Study Done?
This study consisted of two parts:
Part 1 used data from the Alzheimer’s Disease Neuroimaging Initiative (ADNI). The ADNI study is a multicenter study designed to develop clinical, imaging, genetic, and biochemical markers for early detection and tracking of Alzheimer’s Disease.
Participants undergo standardized neuroimaging, psychological assessments, in-person interviews for medical history, and cognitive evaluations on entry into the study and at the end of the study.
This study followed a cohort of 1135 participants (average age = 73, 46% females) without dementia at entry into the study for 6 years.
Omega-3 supplement use was determined based on a questionnaire at the beginning of the study. Participants who used omega-3 supplements for over a year were considered omega-3 users. They were further divided into medium-term users (1-9 years) and long-term users (>10 years).
Alzheimer’s Disease was diagnosed by neurologists based on brain scans, cognitive scores, and the ability to live independently.
Part 2 was a meta-analysis of 31 studies with 103,651 participants. The studies included in the meta-analysis all:
Measured the relationship of omega-3 intake with the risk of Alzheimer’s Disease, all-cause dementia, or cognitive decline.
Were cohort studies (studies that follow a group of people over time) or case control studies (studies that compare people who develop a disease with those who do not).
Provided risk estimates or data that could be used to calculate risk.
Were original publications, not reviews or meta-analyses.
Do Omega-3s Reduce Cognitive Decline?
The results from Part 1 (data from the ADNI study) were as follows:
Omega-3 supplement users had a 37% lower risk of developing Alzheimer’s Disease than non-users.
Long-term (>10 years) omega-3 supplement users fared even better. They had a 64% lower risk of developing Alzheimer’s Disease than non-users.
When they broke the results for long-term omega-3 supplement users into subgroups:
Males (67% risk reduction) benefitted more than females (50% risk reduction).
People over 65 (65% risk reduction) benefited more than those under 65 (22% risk reduction).
People with the APOE ɛ4 genotype (71% risk reduction) benefitted more than those who were APOE ɛ4 negative (55% risk reduction).
The results from Part 2 (data from the meta-analysis) were as follows:
Dietary omega-3 intake lowered the risk of cognitive decline by 9%.
People with the APOE ɛ4 genotype fared better (17% risk reduction).
Their data suggested that a threshold of 1 gm/day omega-3s was needed before significant risk reduction was seen.
Dietary DHA intake lowered the risk of dementia by 27% and Alzheimer’s Disease by 24%.
Each 100 mg/day increase in DHA and EPA was associated with a significant reduction in the risk of cognitive decline (8% for DHA and 9.9% for EPA).
The authors concluded that,
1) “Long-term omega-3 supplementation may reduce risk of Alzheimer’s Disease; and
2) Dietary omega-3 fatty acid intake, especially DHA, may lower risk of dementia or cognitive decline…
3) However, further investigation is needed to understand the gene environment interactions involved in…[these effects of omega-3 fatty acids].”
Should You Supplement With Omega-3s?
This study provides strong support for the hypothesis that omega-3 supplementation reduces the risk of cognitive decline, dementia, and Alzheimer’s Disease as we age. It also suggests that a dose of 1 gram/day may be needed to obtain a significant benefit.
However, it also highlights the difficulty in designing definitive experiments to test this hypothesis. This study shows that gender, age, genetics (especially the APOE ɛ4 genotype), type of omega-3s, dosage, and duration of supplementation all exert a significant influence on the effect of omega-3s on cognitive decline.
It is extremely difficult to design a study that optimizes all these variables, which almost guarantees that the effect of omega-3s on cognitive decline will remain controversial for the foreseeable future.
However, omega-3s lower blood pressure, lower triglycerides, reduce inflammation and are heart-healthy. And the threshold for all these effects is around 1 gram/day or more. If omega-3s also reduce cognitive decline, you can consider that a side-benefit.
The Bottom Line
The role of omega-3s in reducing cognitive decline remains controversial. Some studies strongly support their role in slowing cognitive decline while other studies find no effect.
So, the question remains, “Do omega-3s reduce cognitive decline or not?”
A recent study was designed to answer that question. Among other things the study showed:
Omega-3 supplement users had a 37% lower risk of developing Alzheimer’s Disease than non-users.
Long-term (>10 years) omega-3 supplement users fared even better. They had a 64% lower risk of developing Alzheimer’s Disease than non-users.
Dietary DHA intake lowered the risk of dementia by 27% and Alzheimer’s Disease by 24%.
Each 100 mg/day increase in DHA and EPA was associated with a significant reduction in the risk of cognitive decline (8% for DHA and 9.9% for EPA).
The threshold for observing a significant effect of omega-3s on cognitive decline was around 1 gram/day.
This study provides strong support for the hypothesis that omega-3 supplementation reduces the risk of cognitive decline, dementia, and Alzheimer’s Disease as we age. It also suggests that a dose of 1 gram/day may be needed to obtain a significant benefit.
However, it also highlights the difficulty in designing definitive experiments to test this hypothesis. This study shows that gender, age, genetics (especially the APOE ɛ4 genotype), type of omega-3s, dosage, and duration of supplementation all exert a significant influence on the effect of omega-3s on cognitive decline.
It is extremely difficult to design a study that optimizes all these variables, which almost guarantees that the effect of omega-3s on cognitive decline will remain controversial for the foreseeable future.
However, omega-3s lower blood pressure, lower triglycerides, reduce inflammation and are heart-healthy. And the threshold for all these effects is around 1 gram/day or more. If omega-3s also reduce cognitive decline, you can consider that a side-benefit.
For more information on this study read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
When I was still teaching, a physician and I were co-directors of one of the first courses medical students took at UNC. In his opening lecture to these brand-new medical students, one of his pearls of wisdom was the statement, “The only safe drug is a new drug.”
After a pause to let the students think about it, he followed up with, “That’s because the side effects haven’t been discovered yet.”
He would then go on to explain that every drug must go through rigorous clinical trials, and some side effects are discovered then. But some of the most serious side effects aren’t discovered until years later after 100’s of thousands of patients had used the drugs.
Hormone replacement therapy is a perfect example of this principle. Hormone replacement therapy was first introduced in the 1960s. At first it seemed to be an almost miraculous solution to menopausal symptoms.
Millions of women were overjoyed. After all, menopause symptoms can make life miserable. They include:
Hot flashes
Night sweats
Sleep disturbances
Mood swings
Depression
Anxiety
Forgetfulness
Food cravings
Tiredness
Just to name a few. While only 25% of women experience severe symptoms, why would anyone want to experience any of these symptoms?
And doctors were only too happy to oblige. Why not? The known side effects were mild. Why should any woman experience menopause symptoms?
But that was before the dark side of hormone replacement therapy started to emerge.
The Dark Side Of Hormone Replacement Therapy
The popularity of hormone replacement therapy peaked in the 1990s. It was around that time that reports started to emerge suggesting that hormone replacement therapy increased the risk of heart disease and breast cancer. Those risks were confirmed in a major study called the Woman’s Health Initiative that was published in 2002.
That study caused a major shift in how the medical community regarded hormone replacement therapy. Within a few years doctors shifted from recommending hormone replacement therapy for every woman with menopausal symptoms to recommending it only in cases where the symptoms were debilitating and only for the shortest possible time.
The effect on women’s health was huge. In fact, switching from universal hormone replacement therapy to targeted hormone replacement therapy remains the single most effective public health measure for reducing the incidence of breast cancer. It is more effective than any of new drugs and measures to improve breast cancer screening since then.
I wish I could tell you that was the end of the story. But recent studies have suggested that hormone replacement therapy also increases the risk of dementia. Unfortunately, most of those studies have had flaws, so the link between hormone replacement therapy and dementia has remained controversial – until now.
This was done in Denmark and used the Danish health registries. As Americans, you might not be aware of what a rich resource those health registries are. One advantage of socialized medicine is that every aspect of your health is tracked and recorded from cradle to grave.
[I’m not sure I would be comfortable with our government knowing that much about me, but it is a treasure-trove of information if you want to conduct a study like this one.]
The authors used the Danish National Health registries to:
Identify all Danish women aged 50-60 who had no incidence of dementia and were not on hormone replacement therapy as of January 1, 2000.
Identify 5589 women (1.8% of the population) from this group who were diagnosed with dementia between January 1, 2000 and December 31, 2018 and match them with 55,890 controls who remained dementia-free through the end of 2018.
Using the National Prescription registry, they were able to track which women used hormone-replacement therapy, what kind of therapy it was (there are several variations of hormone replacement therapy), and how long they remained on hormone replacement therapy.
The average age at which hormone replacement therapy began was 53, and the average duration of use was 3.8 years. The average age of a dementia diagnosis was 70.
Does Hormone Replacement Therapy Cause Dementia?
When the authors compared women who used an estrogen-progestin combination hormone replacement therapy (the most common kind) with women who never used hormone replacement therapy, the hormone replacement therapy users were:
24% more likely to develop dementia of any kind.
21% more likely to develop late-onset dementia.
22% more likely to develop Alzheimer’s disease.
Longer duration of hormone replacement use was associated with an increased risk of dementia. The increased risk of dementia was:
21% for ≤ 1 year duration.
39% for 8-12 years duration.
74% for > 12 years duration.
The age at which hormone replacement therapy was begun had a slight effect on dementia risk. The increased risk of dementia was:
26% when it was started at age 45-50.
21% when it was started at age 51-60.
Finally, other forms of hormone replacement therapy such as progestin only therapy and vaginal estrogen treatment did not have a statistically significant effect on dementia risk. But it was not clear whether this was due to a smaller sample size or whether it was a true null effect.
The authors concluded, “Menopausal hormone replacement therapy was positively associated with the development of all cause dementia and Alzheimer’s disease, even in women who received treatment at the age of 55 years or younger.”
The Pros And Cons Of This Study
The pros are obvious. This was a large, well-designed study. And its use of the Danish National Health registry and National Prescription registry allowed it to address the dementia risk of hormone replacement therapy in a comprehensive manner.
The cons are also obvious. This was an observational study. It can only show associations, not prove cause and effect. [I should note that it would be impossible to do a double-blind study to prove cause and effect. The size of the population group and the length of time required would make that kind of study unworkable.]
As I have said in previous issues of “Health Tips From the Professor”, the Achilles heel of observational studies is the possibility that a confounding variable (something else about the women who developed dementia) was the true cause of the observed outcome (in this case, increased dementia risk).
The authors did an excellent job of identifying known confounding variables that might have contributed to dementia and statistically correcting for them. However, the authors identified one potential confounding variable I would not have thought of.
In the words of the authors, “Further studies are warranted to determine whether these findings represent an actual effect of menopausal hormone therapy on dementia risk, or whether they reflect an underlying predisposition in women in need of these treatments.”
In case you need a translation, the authors are saying that it is possible that certain women have an underlying disease state or genetic predisposition that makes them very sensitive to menopausal symptoms (which increases the likelihood that they would receive hormone replacement therapy to reduce their symptoms) and increases their risk of dementia. In that case, it would be the underlying medical condition or genetic predisposition that was responsible for the increased dementia risk, not the hormone replacement therapy.”
I consider that unlikely, but it does warrant future studies.
Is Hormone Replacement Therapy Right For You?
Ultimately, this is your decision. But this is a decision you should make with your health care provider.
It is clear that hormone replacement therapy increases your risk of heart disease, breast cancer, and may increase your risk of dementia.
In part, your decision depends on the severity of your symptoms and your willingness to accept the risks associated with alleviating those symptoms.
But your health care provider can also help you consider family history and unrelated health conditions that may also increase your risk of these diseases. If your underlying disease risk is low, would you be more willing or less willing to accept the risks associated with hormone replacement therapy? Again, this is your decision.
And, if you decide to proceed with hormone replacement therapy, your health care provider can recommend the type of therapy and length of therapy that will minimize your risks.
The Bottom Line
Several recent studies have suggested that hormone replacement therapy may increase the risk of dementia, but this has remained controversial.
In this issue of “Health Tips From the Professor” I share a very large, well designed study that supports the link between hormone replacement therapy and dementia.
When the authors of this study compared women who had used hormone replacement therapy with women who never used hormone replacement therapy, the hormone replacement therapy users were:
24% more likely to develop dementia of any kind.
21% more likely to develop late-onset dementia.
22% more likely to develop Alzheimer’s disease.
The authors concluded, “Menopausal hormone replacement therapy was positively associated with the development of all cause dementia and Alzheimer’s disease, even in women who received treatment at the age of 55 years or younger.”
For more information on the strengths and weaknesses of this study and a discussion of whether hormone replacement therapy might be right for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Author: Julie Donnelly, LMT – The Pain Relief Expert
Editor: Dr. Steve Chaney
The holidays are inching up on us, and this month is one of my favorites. I love Halloween because the children have so much fun dressing up and going to parties.
Back when I was a child we could roam around the neighborhood, knocking on doors and having our candy dropped into the pumpkin basket or pillowcase our moms gave us. We traveled in a pack, and our parents knew we were safe as long as we stayed in our neighborhood because everyone knew everyone.
Nowadays children go to “Trunk or Treat” parties, often with mom or dad in tow. They’re still having fun, and it’s great to see their excitement when they’re sharing with each other how many goodies they have collected.
Now, even just LOOKING at that candy makes me gain 5 lbs! Oh well!
Happy October to you and your family!
Your Pectineus Muscle And Groin Pain
Today, we will be discussing how a small muscle that most people aren’t even aware of can cause groin pain. I’ve been working with athletes since 1989 and I’ve seen this small muscle cause such pain that it was preventing the athlete from continuing with his/her sport. And it’s so simple to treat!
The pectineus muscle is in your adductor muscle group. The adductors are responsible for hip flexion and adduction.
Adduction is when you bring your leg closer to the opposite leg, such as when you cross your legs when you are sitting down. Athletes who play soccer, or who ride a horse, are heavily using their adductor muscles.
As you look at the graphic on the left, the muscles on the left side (right leg) are the larger adductor muscles.
The pectineus is shown on the right side (left leg) so that it is more visible, helping you see the location of the muscle. In reality, all the muscles are on both sides.
Since the pectineus muscle is so close to the pubic bone, it is more difficult to self-treat. You need to sit on the floor and twist yourself, so the sore side is pressing into the floor.
The pectineus muscle is often overlooked, but it can cause significant pain when in spasm or injured. Here are some of the symptoms, causes, and a simple self-treatment I have developed for a tight pectineus.
Quick Facts About Groin Pain And Your Pectineus Muscle
Causes of Spasms of the Pectineus and Adductors:
Muscular injuries of the adductors, the iliopsoas muscle, and abdominal musculature are the most frequent causes of acute groin pain in sportsmen and sportswomen.
Spasms in your pectineus muscle are also a common cause of groin pain and are often overlooked.
Pectineus pain often stems from an injured groin muscle. Common causes include running, kicking a soccer ball, riding a horse, and sitting with a crossed leg.
Symptoms Of Groin Pain Caused By Your Pectineus Muscle:
Groin pain is any discomfort in the area between your abdomen and thigh, located where your abdomen ends, and your legs begin.
Localized pain on the pubic bone, in the groin area, on one side or the other, is a primary indication of injury to the pectineus.
Pain on palpation of the involved muscle and pain on adduction (moving your legs closer together against resistance) is also an indication of injury to the pectineus.
Treating Groin Pain Naturally
You are trying to be pressing close to your pubic bone, which is shown in the graphic above.
Sit as shown and use a ball to press deeply into your adductors. Start the treatment at the very top of the muscles, close to your pubic bone, and move down toward your knee.
If you find any tender points, called “trigger points,” hold the pressure on the spasm until it stops hurting.
You can also “pump” the trigger point, applying pressure for 15 seconds, then stay where you are but release the pressure for 5 seconds, and repeat this sequence several times until the pain point stops hurting.
You may get better leverage if you lift up your opposite hip (lift up the right hip in this demonstration), bending your right leg so you can press your right elbow into your thigh to get better pressure.
If it’s difficult with the ball, use your right hand fingertips to press on the muscle on your left side.
In conclusion, the pectineus muscle can cause groin pain when injured.
If this simple self-treatment doesn’t help, it would be important to seek medical attention to determine the underlying cause, especially if it is severe or accompanied by other symptoms.
Wishing you well,
Julie Donnelly
www.FlexibleAthlete.com
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
 While February is the shortest month of the year, to our northern family and friends it is the longest, seemingly endless, month because it seems like winter is never going to go away.
While February is the shortest month of the year, to our northern family and friends it is the longest, seemingly endless, month because it seems like winter is never going to go away.
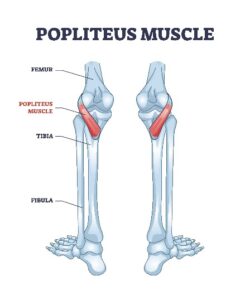 The popliteus is a small muscle that causes a LOT of deep-knee pain. It is located at the back of your knee joint. It attaches to the bone in your lower leg, crosses the joint, and inserts into your thigh bone. You can get a good look at it and read all about it by going to https://en.wikipedia.org/wiki/Popliteus_muscle.
The popliteus is a small muscle that causes a LOT of deep-knee pain. It is located at the back of your knee joint. It attaches to the bone in your lower leg, crosses the joint, and inserts into your thigh bone. You can get a good look at it and read all about it by going to https://en.wikipedia.org/wiki/Popliteus_muscle. This book has been called “the bible” by athletes because they could find all their answers in it.
This book has been called “the bible” by athletes because they could find all their answers in it. Julie Donnelly has been a licensed massage therapist since 1989, specializing in the treatment of chronic pain and sports injuries. The author of several books including Treat Yourself to Pain-Free Living, The Pain-Free Athlete, and The 15 Minute Back Pain Solution.
Julie Donnelly has been a licensed massage therapist since 1989, specializing in the treatment of chronic pain and sports injuries. The author of several books including Treat Yourself to Pain-Free Living, The Pain-Free Athlete, and The 15 Minute Back Pain Solution.