Should You Follow Your Doctor’s Advice About Calcium Supplementation?
Author: Dr. Stephen Chaney
 Are calcium supplements good for your heart or bad for your heart? If you don’t know the answer to that question, don’t feel badly. You have every right to be confused. Some studies say that calcium supplements increase heart disease risk while others say they decrease heart disease risk. The headlines have veered between “killer calcium” and “beneficial calcium”.
Are calcium supplements good for your heart or bad for your heart? If you don’t know the answer to that question, don’t feel badly. You have every right to be confused. Some studies say that calcium supplements increase heart disease risk while others say they decrease heart disease risk. The headlines have veered between “killer calcium” and “beneficial calcium”.
The trend appears to be moving in a positive direction. In recent years most of the studies have suggested that calcium supplements either decrease heart disease risk or have no effect on heart disease risk.
However, the medical profession has been slow to take note of this trend. Most medical societies and health professionals have focused on earlier studies and are still recommending that their patients get calcium from food rather than from supplements. I will talk more about that recommendation below.
With this context in mind, this week I will review and discuss the results from the latest study (MG Sim et al, Heart, Lung and Circulation, 32: 1230-1239, 2023) on the effect of calcium supplementation on heart disease risk.
How Was This Study Done?
 The authors of this study performed a meta-analysis of 12 double-blinded randomized clinical trials with 87,899 participants comparing the effect of a calcium supplement versus a placebo on heart disease outcomes (heart attack, stroke, heart failure, cardiovascular mortality, and all-cause mortality).
The authors of this study performed a meta-analysis of 12 double-blinded randomized clinical trials with 87,899 participants comparing the effect of a calcium supplement versus a placebo on heart disease outcomes (heart attack, stroke, heart failure, cardiovascular mortality, and all-cause mortality).
The studies included in this analysis:
- Used calcium doses from 500 mg/day to 2,000 mg/day.
- Used supplements with calcium coming from a variety of sources (calcium carbonate, calcium citrate, calcium gluconolactate, and tricalcium phosphate).
- Ranged from 18 months to almost 12 years in length.
- Were performed with population groups from a wide range of countries (United States, England, France, Australia, New Zealand, European Union, Denmark, and Thailand).
- Included calcium supplements with and without vitamin D.
- Were primarily (86% of participants) conducted with post-menopausal women. One small study (0.3% of participants) was conducted with non-osteoporotic men. The rest were conducted with mixed populations (men and women) diagnosed with colorectal adenoma.
Are Calcium Supplements Heart Healthy?
 This is the largest meta-analysis performed to date of double-blind, placebo-controlled randomized clinical trials on the effect of calcium supplementation versus a placebo on heart disease outcomes. This study found no effect of calcium supplementation on:
This is the largest meta-analysis performed to date of double-blind, placebo-controlled randomized clinical trials on the effect of calcium supplementation versus a placebo on heart disease outcomes. This study found no effect of calcium supplementation on:
- Heart attack.
- Stroke
- Heart failure.
- Cardiovascular mortality.
- All-cause mortality.
This study also evaluated potential confounding variables and found no effect of calcium supplementation on heart disease risk for:
- Calcium supplements with and without vitamin D.
- Dosage of calcium in the supplements (The dosage ranged from 500 mg/day to 2,000 mg/day).
- Females (I suspect the number of males in this study was too small to come to a statistically significant conclusion).
- Duration of calcium supplementation ≤ 5 years (The shortest duration of calcium supplementation in these studies was 18 months).
- Different geographical regions.
However, this meta-analysis reported considerable variation between studies included in the analysis. Simply put,
- Some studies showed an increase in heart disease risk.
- Some studies showed a decrease in heart disease risk.
- Some studies showed no effect on heart disease risk.
What this analysis showed was that when you combine all the studies, the aggregated data is consistent with calcium supplementation having no effect on heart disease risk.
The authors concluded, “Calcium supplementation was not associated with myocardial infraction [heart attack], stroke, heart failure, and cardiovascular/all-cause mortality. Further studies are required to examine and understand these associations.
Should You Follow Your Doctor’s Advice About Calcium Supplementation?
 As I said above, most medical societies and health professionals have focused on earlier studies and are still recommending that their patients get calcium from food rather than from supplements. That may be the advice you are getting from your doctor.
As I said above, most medical societies and health professionals have focused on earlier studies and are still recommending that their patients get calcium from food rather than from supplements. That may be the advice you are getting from your doctor.
Before you assume your doctor isn’t keeping up with the latest science and ignore his or her advice, we should ask why they are giving that advice. The top three reasons most medical societies give for recommending dietary sources of calcium are:
1) Some studies do show an increased risk of heart disease associated with calcium supplementation. The prime directive for health professionals is to do no harm. Yes, the average of all studies shows no effect of calcium supplementation on heart disease risk. But what if the studies showing increased risk are true for some of their patients? Those patients could be harmed.
Are you someone who might be at increased risk for heart disease if you take calcium supplements. The short answer is we don’t know because previous studies have not asked the right questions.
In my opinion, it is time to pause additional studies and meta-analyses on calcium supplementation and heart health until we have gone over existing studies with a fine-tooth comb to figure out why the results differ so wildly. For example, we need to ask whether the effect of calcium supplements on heart disease risk is influenced by things like:
-
- Age or ethnicity of participants.
-
- Other preexisting health conditions.
-
- Other lifestyle factors (exercise is probably the most important, but others may be involved as well).
-
- Diet context. For example, we already know that the effect of eggs and dairy on heart health is influenced by diet context. [I have covered this for eggs in a previous issue of “Health Tips From the Professor”.]
-
- Other unanticipated variables.
Only when we have identified variables that might influence the effect of calcium supplements on heart disease risk, will the scientific community be able to design studies to identify the population groups who might be adversely affected by calcium supplementation.
This would allow health professionals to make informed decisions about which of their patients should avoid calcium supplementation and which of their patients would benefit from calcium supplementation.
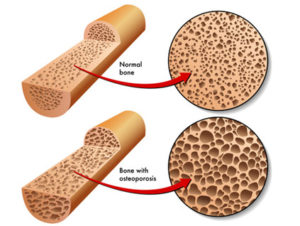
2) We really don’t need the recommended RDAs for calcium to build strong bones. The  recommended RDAs for calcium are 1,000 mg/day for adults 19-50, 1,000 mg/day for men and 1,200 mg/day for women 51-70, and 1,200 mg/day for both men and women over 70. But do we really need that amount of calcium to build healthy bones?
recommended RDAs for calcium are 1,000 mg/day for adults 19-50, 1,000 mg/day for men and 1,200 mg/day for women 51-70, and 1,200 mg/day for both men and women over 70. But do we really need that amount of calcium to build healthy bones?
I have discussed this topic in detail in a previous issue of “Health Tips From the Professor”. Here are the key points:
-
- The current RDAs are based on calcium needs for people consuming the typical American diet and following the typical American lifestyle. If that is you, the current RDAs probably apply.
-
- However, strong bones are absolutely dependent on three things, adequate calcium, adequate vitamin D, and adequate weight-bearing exercise. Most recent studies of calcium supplementation and bone density include adequate vitamin D, but almost none of them include exercise. Previous studies have been inadequate.
-
- The best calcium supplements contain certain nutrients besides vitamin D that optimize bone formation. I have listed those nutrients in the article cited above.
-
- Our ability to use calcium to build strong bones is dependent on diet (something I call a bone-healthy diet) and lifestyle (something I call a bone-healthy lifestyle).
-
- For more information on each of these points, read the article I referenced above.
In short, I agree that the current calcium RDAs may be too high for individuals consuming a bone-healthy diet and following a bone-healthy lifestyle. But the current calcium RDAs are likely accurate for people consuming the typical American diet and following the typical American lifestyle.
-
- While we do not have a calcium RDA for populations following a bone healthy diet lifestyle, some studies suggest that 700-800 mg of calcium/day may be sufficient for this group.
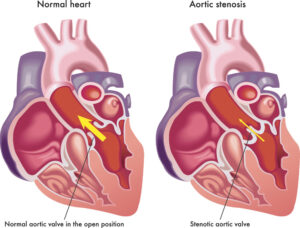
 3) Calcium from supplements is absorbed faster and gives higher blood level spikes than calcium from foods. That could be a problem because high blood levels of calcium are associated with calcification of our arteries, which is associated with increased heart disease risk.
3) Calcium from supplements is absorbed faster and gives higher blood level spikes than calcium from foods. That could be a problem because high blood levels of calcium are associated with calcification of our arteries, which is associated with increased heart disease risk.
This is a theoretical concern, because high blood calcium levels from supplementation are transitory, while it is continuous high blood calcium levels that are associated with calcification of our arteries.
However, it is a plausible concern because most supplement companies design their calcium supplements based on how quickly they get calcium into the bloodstream rather than how effectively the calcium is utilized for bone formation. Here are my recommendations:
-
- Choose a calcium supplement that provides RDA levels of vitamin D plus other nutrients shown to support strong bone formation.
-
- Choose a calcium supplement supported by clinical studies showing it is effectively utilized for bone formation.
4) We should be getting our calcium from foods rather than supplements. 
While it is always easy for doctors to recommend that we get our nutrients from food rather than supplements, they need to ask whether we are getting those nutrients from our diet. For calcium the data are particularly sobering.
-
- The average American gets around 740 mg of calcium/day from their diet. That is probably enough for the small percentage of Americans following a bone healthy diet and lifestyle. But it is 260-460 mg short of the 1,000-1,200 mg/day recommended for older adults with the typical American diet and lifestyle.
-
-
- And for the average American, around 70% of their calcium intake comes from dairy foods.
- So, Americans who are following a typical American diet and lifestyle and are restricting dairy may require 800-1,000 mg/day of supplemental calcium unless they carefully plan their diets to optimize calcium intake.
- Finally, vegans average about 550 mg/day from their diet. That might be borderline even if they were following a bone healthy lifestyle.
-
-
- In short, we cannot assume our diet will provide enough calcium for strong bones unless we include dairy foods and/or plan our diet very carefully. Some degree of supplementation may be necessary.
How Much Calcium Do You Need?

I have covered a lot of territory in this article, so let me summarize the four concerns of the medical community and answer your most important question, “Should you take calcium supplements?”
1) Calcium supplements may increase the risk of heart disease for some people.
That is true, but we have no idea at present who is at increased risk and who isn’t. So, we should minimize our risk by taking the precautions I describe below.
2) We don’t need RDA levels of calcium to build strong bones. That is probably true if you are one of the few people who follows a bone healthy diet and lifestyle, but it isn’t true if you follow the typical American diet and lifestyle.
- The current RDAs of 1,000 – 1,200 mg/day are a good guideline for how much calcium you need if you follow the typical American diet and lifestyle.
- If you a one of the few people who follow a bone healthy diet and lifestyle (For what that involves, read this article) you may only need 700-800 mg/day. But we don’t have clinical studies that can tell us what the actual RDA for calcium should be under those circumstances.
3) Calcium from supplements is absorbed faster and gives higher blood calcium spikes than calcium from foods. You may remember that the theoretical concern is that even short-term spikes of high blood calcium may lead to calcification of your arteries, which increases your risk of heart disease. So, the important question becomes, “What can we do to minimize these spikes in blood calcium levels?”
- We should avoid calcium supplements that brag about how quickly and efficiently the calcium is absorbed. That could lead to calcium spikes. Instead, we should look for calcium supplements that are backed by clinical studies showing they are efficiently utilized for bone formation.
- We should look for calcium supplements that include RDA levels of vitamin D and other nutrients that optimize bone formation. You will find more information on that in the same article I referenced above.
- Some experts recommend that calcium supplements be taken between meals. But it is probably better to take them with meals because foods will likely slow the rate at which calcium is absorbed and reduce calcium spikes in the blood.
- We are told to limit calcium supplements to less than 500 mg at any one time because calcium absorption becomes inefficient at higher doses. It might be even better to limit calcium to 250 mg or less at a time to reduce calcium spikes in the blood.
4) We should get calcium from foods rather than supplements.
- Many Americans do not get enough calcium from diet alone, especially if they avoid dairy foods. So, some degree of calcium supplementation may be necessary. I have given some guidelines depending on your diet and lifestyle above.
- The amount of supplemental calcium needed is relatively small. I do not recommend exceeding the RDA unless directed to by your health professional.
The Bottom Line
Some studies say that calcium supplements increase heart disease risk while others say they decrease heart disease risk. The headlines veer between “killer calcium” and “beneficial calcium”.
The trend appears to be moving in a positive direction. In recent years most of the studies have suggested that calcium supplements either decrease heart disease risk or have no effect on heart disease risk.
However, the medical profession has been slow to take note of this trend. Most medical societies and health professionals have focused on earlier studies and are still recommending that their patients get calcium from food rather than from supplements.
A recent meta-analysis of 12 double-blinded randomized clinical trials with 87,899 participants comparing the effect of a calcium supplement versus a placebo on heart disease outcomes has just been published. This study found no effect of calcium supplementation on:
- Heart attack.
- Stroke.
- Heart failure.
- Cardiovascular mortality.
- All-cause mortality.
The authors of the study concluded, “Calcium supplementation was not associated with myocardial infraction [heart attack], stroke, heart failure, and cardiovascular/all-cause mortality.
For more details and advice on whether you should follow your doctor’s recommendations for calcium supplementation read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
_____________________________________________________________________________
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
https://www.ftc.gov/business-guidance/resources/health-products-compliance-guidance
____________________________________________________________________
About The Author
 Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.