Author: Dr. Stephen Chaney
 Is there a connection between calcium and breast cancer prevention? There has been lots of confusion about calcium supplements lately. Just a few years ago most health professionals were recommending calcium supplementation for women to prevent osteoporosis. Now that recommendation has become controversial. That’s because some studies have suggested that increasing calcium intake doesn’t actually prevent osteoporosis. Other studies have suggested that calcium supplementation may actually cause heart disease.
Is there a connection between calcium and breast cancer prevention? There has been lots of confusion about calcium supplements lately. Just a few years ago most health professionals were recommending calcium supplementation for women to prevent osteoporosis. Now that recommendation has become controversial. That’s because some studies have suggested that increasing calcium intake doesn’t actually prevent osteoporosis. Other studies have suggested that calcium supplementation may actually cause heart disease.
As if all this wasn’t confusing enough, the latest headlines are claiming that increased calcium intake will reduce breast cancer risk. What are we to believe about the value of calcium for our health? Should we take that calcium supplement we threw away out of the trash can and start using it again?
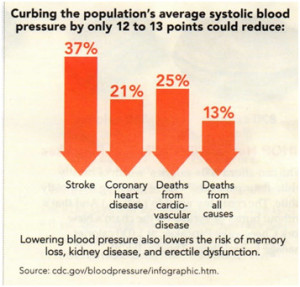
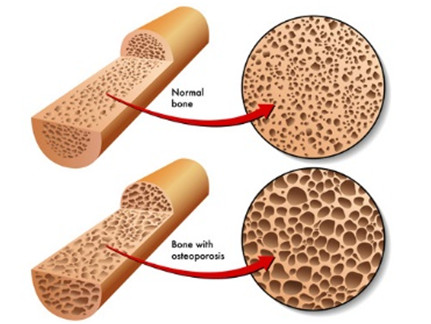
I have previously evaluated the studies behind the previous headlines and debunked the headlines. For example, I reported that previous studies suggesting that calcium supplementation might increase heart attack risk were followed by a much larger, better designed study showing that, if anything, calcium supplementation actually decreases heart attack risk in Do Calcium Supplements Increase Heart Attack Risk?. I also reported that the study claiming calcium supplements did not prevent osteoporosis was fatally flawed in Do Calcium Supplements Prevent Bone Fractures?.
Now it is time to evaluate the study behind the latest calcium headline. Is this headline myth or is it true? What is the connection between calcium and breast cancer.
Calcium and Breast Cancer Risk Reduction
 This study (Hidayat et al, British Journal of Nutrition, 116: 158-166, 2016) was a meta-analysis of 11 previous clinical studies published between 2002 and 2013 with a total of 872,895 women subjects which measured calcium intake and breast cancer. Follow up ranged from 7 to 25 years in these studies, during which time 26,606 of the women developed breast cancer.
This study (Hidayat et al, British Journal of Nutrition, 116: 158-166, 2016) was a meta-analysis of 11 previous clinical studies published between 2002 and 2013 with a total of 872,895 women subjects which measured calcium intake and breast cancer. Follow up ranged from 7 to 25 years in these studies, during which time 26,606 of the women developed breast cancer.
Dietary plus supplemental calcium intake was determined at the beginning of each study using either a 24-hour diet recall or a food frequency questionnaire. Calcium intakes ranged from 203 mg/day to 1,750 mg/day.
In short this was a very large and well done study. Because of the large number of subjects and the large number of cancer cases, this study had the sensitivity to detect even small effects of calcium on breast cancer risk – something that was not possible in previous studies. In addition, the investigators were able to conduct a dose-response evaluation of the effect of calcium and breast cancer risk reduction. This was also had not been possible in previous studies.
When the women with the highest calcium intakes were compared to the women with the lowest calcium intakes:
- Calcium reduced breast cancer risk by 8%.
- The effect was much larger for premenopausal women than postmenopausal women:
- Calcium reduced breast cancer risk by 25% in premenopausal women.
- Calcium reduced breast cancer risk by 6% in postmenopausal women.
- The dose response effect was fairly linear over the entire dose range with a 2% decreased risk of breast cancer for every 300 mg/day increase in calcium intake.
What Does This Study Mean For You?
As I said in the beginning, when you read the headlines proclaiming that increasing your calcium intake could decrease your breast cancer risk, you probably had two questions:
Is it true? The answer appears to be yes. This was a very large, very well done study and it showed there is a connection between calcium and breast cancer risk reduction. It was capable of detecting even small effects of calcium on breast cancer risk – something that previous studies simply could not do.
Does it matter? Here the answer is more complicated. If you’re a postmenopausal woman, increased calcium intake only decreases your risk of breast cancer by 6%. If you are a premenopausal woman, increased calcium intake decreases your risk of breast cancer by a more robust 25%. However, in both cases you should think of calcium as only one component of a holistic approach to reducing breast cancer risk – something I’ll discuss in more detail below.
Now that you know the answer to those two questions you probably have a third question:
How much calcium do I need? That’s pretty simple. The calcium DV for adults is 1,000 mg/day, increasing to 1,200 mg/day for women over 50.
How Can You Reduce Breast Cancer Risk?
In a previous article Preventing Osteoporosis, I reported that while calcium supplementation alone had only a very modest effect on reducing osteoporosis risk, it played an important role as part of a holistic bone-healthy lifestyle. The role of calcium in reducing breast cancer risk is no different.
Most experts estimate that between 30 and 60% of breast cancer cases could be prevented by diet and lifestyle changes. In addition to calcium, both the Mayo Clinic and the American Cancer Society make the following recommendations for reducing breast cancer risk:
 Limit or avoid hormone therapy. This is the single most important step you can take to reduce breast cancer risk.
Limit or avoid hormone therapy. This is the single most important step you can take to reduce breast cancer risk.
- Eat a plant-based diet with plenty of fresh fruits and vegetables, whole grains, legumes and nuts. Use fats in moderation and choose healthy fats such as olive oil and omega-3 fats. Limit the amounts of red meat and processed meats.
- Control your weight.
- Be physically active.
- Don’t smoke
- Limit alcohol intake.
- Avoid exposure to radiation and environmental pollution.
- Breast feed.
Where Should You Get Your Calcium?
Many experts recommend that you get your calcium only from food. Is that the best advice? I always like to start with food as the source of essential nutrients, but in the case of calcium that usually isn’t sufficient. Here are some facts to ponder:
- Plain, nonfat yoghurt is the calcium champion, with an 8 ounce serving supplying 42% of the DV (the calcium DV = 1,000 mg/day). However, most yoghurt cups in the market these days are 4 ounces or less.
- Milk and a few cheeses supply around 30% of the DV. However, many people can’t or don’t consume the 3 or more servings needed to reach the DV.
- Green leafy vegetables are often mentioned as another good food source. However, a serving of them only provides around 10% of the DV, and many leafy greens contain oxalates which decrease calcium absorption.
- Beyond that, most food sources of calcium supply only 1-8% of the DV for calcium. If you don’t drink lots of milk, you need to be a dietitian with an advanced degree to figure out how to get enough calcium from foods alone.
- If that isn’t bad enough, many foods contain substances that interfere with calcium absorption. In addition to the oxalates in leafy greens, these substances include phytates from whole grains, phosphate from sodas, and saturated fat from red meats.
Experts often also recommend getting calcium from calcium fortified foods such as calcium fortified orange juice. That can help you reach the recommended calcium intake, but in my opinion calcium-fortified foods are likely to be more expensive and no better than regular foods plus a calcium supplement.
I recommend getting as much calcium as possible from food and adding a calcium supplement for the rest. Here are my tips on calcium supplementation:
- If you do use a calcium supplement, make sure it is complete. Don’t just settle for calcium and vitamin D. At the very least you will want your supplement to contain magnesium and vitamin K. I personally recommend that it also contain zinc, copper, and manganese as well.
- Your calcium supplement will be best utilized if taken between meals.
- Your calcium supplement will be best utilized if you don’t take more than 500 mg at a time.
- In most cases there is no need for more than the DV of calcium.
Let’s review the connection between calcium and breast cancer risk reduction.
The Bottom Line
- A recent study has shown that increasing calcium intake reduces the risk of breast cancer. The effect of calcium intake on breast cancer risk was much greater for premenopausal women (25% risk reduction) than it was for postmenopausal women (6% risk reduction).
- While the effect of calcium alone on breast cancer risk was relatively modest, it is likely to be an important component of a holistic approach for reducing breast cancer risk. Additional recommendations of the Mayo Clinic and American Cancer Society for reducing breast cancer risk are contained in the article above.
- While many experts recommend getting your calcium from food alone, a careful analysis of food sources of calcium clearly shows how difficult that is for most people.
- Calcium supplements are a safe and effective way to make sure you are getting the calcium you need. In the article above, I describe the optimal design of a calcium supplement and how to take a calcium supplement for optimal utilization.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.